Indian Journal of Physiology
and Pharmacology
and Pharmacology
Indian Journal of Physiology and Pharmacology |
 (252x320).jpg) |
Volume 58 - Number 2 April - 2014 (Current issue) ISSN 0019-5499 |
Pulmonary Function Parameters in Workers of Woolen IndustryRitu Purohit, Hem Lata, Lily Walia and Jagdeep Whig |
There is an increase in proportion of workers suffering from occupational diseases. In occupational respiratory diseases, pulmonary function tests are the most important and widely used diagnostic tool. Limited studies have been conducted to evaluate the effect of wool dust on pulmonary function parameters. Hence, the present study was undertaken to evaluate the pulmonary function parameters in workers of woolen industry. This study was done on 150 subjects of either gender who were divided into two groups of 75 each. Group I comprised of healthy subjects who served as controls and group II included workers of woolen industry. The values of lung function parameters i.e. volumes and flow rates in these workers were found to be lower than the healthy controls. The significant reduction in percentage predicted values of FEV (82 vs 59), FVC (79 vs 63) and MVV (77 vs 64) in workers as compared to healthy controls indicates obstructive pattern of respiratory abnormality. In male workers, percentage predicted FEV1 % was significantly lower. The values of all other parameters were lower in female workers. There was a significant decrease in FEV1 and FVC with increase in age in group I and this negative correlation was statistically significant. The decrease in respiratory volumes and flow rates was more with increase in duration of exposure to wool dust. It can be concluded that wool dust present in environment of woolen industry affected the pulmonary function parameters of the workers leading to obstructive pattern of respiratory changes. |
The industrial population is exposed to various types of pollutants present in their working environment leading to occupational diseases (1, 2). A large extent of the workers engaged in these environments are exposed to trace metals, gases, wool dust and cotton dust which can lead to unhealthy manifestations on the vital systems of the body. Respiratory system suffers the most due to its direct communication with the external environment (3). There is increased prevalence of respiratory diseases in these workers. Occupational diseases affecting respiratory system include chronic bronchitis, emphysema and bronchial asthma. The type of work and duration of exposure influences respiratory morbidity among these workers (4). In India, the total work force in industries was six million in 1986. However, due to tremendous mushrooming of industries the workforce has increased to 62 million now (5). Pulmonary function tests are essential to assess the pulmonary function status and respiratory efficiency in these workers. These tests have assumed a key role in epidemiological studies investigating the incidence, natural history and causality of occupational respiratory diseases (6). In occupational respiratory diseases, spirometry is one of the most important diagnostic pulmonary function tests. Spirometry appears to be simple and inexpensive method to measure disorders of respiratory tract (7). Typical changes in major pulmonary function parameters like FEV1, FVC FEV1 % and PEFR can indicate the type of respiratory pathology and the extent of severity (8, 9). Percentage predicted value of these parameters is considered to be better indicator of respiratory disorders (10, 11). Periodic testing and re-testing of workers can detect pulmonary disease in its earliest stages when corrective measures are more likely to be beneficial (4). The limited number of studies conducted in workers of woolen industry in India and other countries have commented on few parameters only and not commented appropriately on the effect of duration of exposure and various others aspects. These studies reported mild and inconsistent effects on lung volumes in workers of woolen industry. Most of these studies commented mainly on the existence of respiratory symptoms and few lung volumes or capacities in workers exposed to airborne wool dust. There is less data on predicted and percentage predicted pulmonary function parameters in workers of woolen industry. Although these studies reported the effect of duration of exposure and dust concentration on some lung volumes, these studies in their limitations mentioned inaccuracies in calculating above factors (12-14). Hence, this study was planned to evaluate the changes in pulmonary function parameters in workers of woolen industry. |
The study was conducted in 150 subjects in the department of Physiology. Subjects were divided into 2 groups consisting of 75 subjects in each group. Group I included healthy subjects who served as control group and group II included workers working in woolen industry. All these subjects were in the age range of 18-60 years and working in same shift i.e. morning shift. Subjects who were smokers or on any medication, who were suffering from respiratory disorders before joining factory or suffering from cardiac diseases or who had chest deformity or who have undergone recent eye, abdominal or thoracic surgical procedures or who had history of syncope associated with forced exhalation were excluded from the study. The study was approved by institutional ethics committee. Study procedure Subjects who fulfilled the inclusion criteria were enrolled into the study after they signed a written informed consent. All the subjects were examined and their vitals were recorded. Height, weight and body surface area (BSA) affect the lung function parameters hence, these were measured (15). Body height was noted in standing upright position without shoes in centimeters (cms). Body weight was measured in kilograms (Kgs) and then body surface area (BSA) was calculated (1). Pulmonary function parameters were measured using spirometry with the help of a computerized autospirometer (Helios 701: Chandigarh). It had an inbuilt printer which gave print outs containing subject's information and calculated values of all parameters. The handset is designed in such a way that it is easy to be used by persons of all ages. All the subjects were thoroughly acquainted with the apparatus and were explained the maneuvers to perform the tests as per standard guidelines (16). All the subjects were instructed not to have a heavy meal before the test. The subjects were also explained that they might have some temporary shortness of breath or light headedness after these tests involving rapid and forced breathing. The subjects were instructed to loosen any tight clothing. The tests were carried out in standing posture. A nose clip was attached to the subject and a clean mouth piece was inserted into the breathing tube. It was made sure that there was no air leakage around the mouth piece and nose. Subject was asked to inspire maximally and to put in his best efforts during expirations as well. In the procedure 1, subjects were asked to inspire maximally from end expiratory position, then to place mouthpiece firmly in mouth, expire as hard, deep, rapid and completely as possible and then remove mouth piece. The parameters recorded automatically by autospirometer included: Forced vital capacity FVC(L); Forced expiratory volumes over fixed time intervals (in seconds)-FEV0.5 , FEV1 , FEV (L); Maximum mid expiratory flow rate - FEF25-75% (L/sec); Mean forced expiratory flow rate between 0.2 to 1.2 litres of volume change-FEF0.2-1.2 (L/sec); Peak expiratory flow rate-PEFR (L/sec); Forced expiratory flow after 25% of the FVC has been expired FEF25% (L/sec); Forced expiratory flow after 50% of the FVC has been expired-FEF50%(L/sec); Forced expiratory flow after 75% of the FVC has been expired-FEF75% (L/sec); Forced expiratory volume (timed) to forced vital capacity ratio expressed as percentage i.e. FEV0.5%, FEV1.0% and FEV3.0 After rest of 5 minutes, subject was asked to breathe as rapidly and deeply as possible in and from the mouth piece for 15 seconds (procedure 2). This provided measurement of maximum voluntary ventilation (MVV) (6, 7, 15). The decrease in MVV is an indicator of increase in airway resistance. Apart from the absolute values of these parameters measures, predicted and percentage predicted values were derived for FEV1, FVC, FEV1 % and FEF25-75%, FEF0.2-1.2 PEFR and MVV using regression equation for Indian subjects. The regression equation developed for eastern Indian region was used as it is reported to give results similar to north Indians. However, this equation has been used in males only, so we used it for male subjects in our study (17). As we could not find appropriate regression equation for north Indian females, we used equation available for south Indians females (11, 18). However, for FEF0.2-1.2, and MVV, predicted values were calculated for male subjects only as no corresponding appropriate equation was available for females. This was followed by calculation of percentage predictive values for these parameters. The FEV1/FVC ratio was calculated, which is considered to be gold standard for diagnosing obstructive disorders (17). Statistical analysis was done by using independent 't' tests for comparison of pulmonary function parameters. ANOVA followed by Posthoc test for multiple comparisons was applied for comparing various pulmonary function parameters within the groups. Comparison of various lung function variables with duration of exposure in years in group II subjects was also done. Subgroup analysis was done for various age groups and gender using factorial ANOVA. P<0.05 was considered as statistically significant. Pearson’s correlation coefficient was used for assessing relationship between anthropometric parameters and various pulmonary function parameters. |
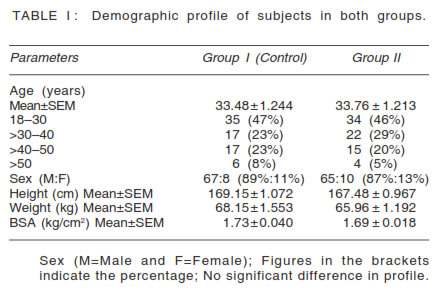
The demographic profile of subjects was comparable
in both groups (Table I). Males comprised 89% of
the subjects in group I and 87% in group II. Forty
seven (47%) of subjects in group I and 46% of
subjects in group II were in the age group of 18-30
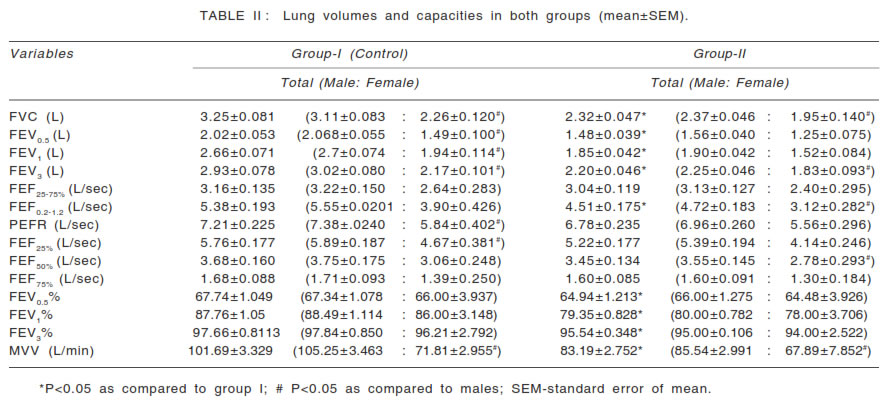
years. Table II shows various lung volumes and
capacities recorded by autospirometery. The values
of FEV1,
FEV1 % and FVC in group II was lower than
that of group I and it was statistically significant.
Similarly FEV0.5, FEV3.0,
FEF0.2-1.2,
FEV0.5%, FEV3.0% and
MVV
were significantly lower in group II than in group
I. The mean values of PEFR, FEF25-75%, FEF50%, FEF75% were also lower in group II than in group I, however
the difference was not statistically significant.
The
values of all the parameters in females were lower
as compared to males in both the groups. There
was a significant reduction in percentage predicted
FEV
FVC and MVV in workers (group II) as
compared to group I (Table III). There was decrease in percentage predicted FEV1%, FEF25-75% and PEFR,
but it was not statistically significant. Gender based
comparison shows significant decrease in percentage
predicted FEV1 % in males in group I. |
 |
 |
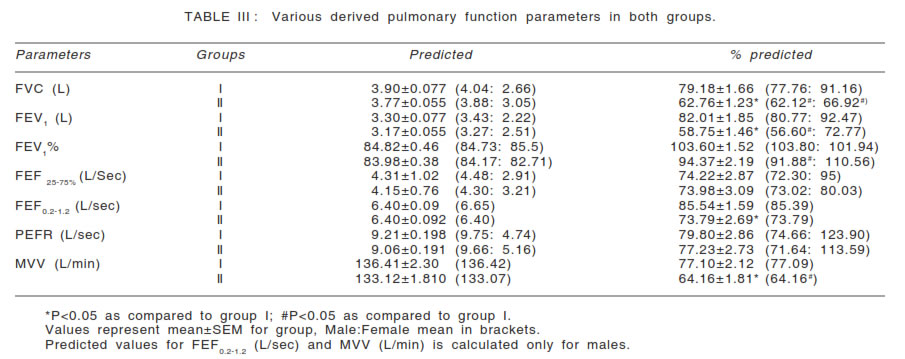 |
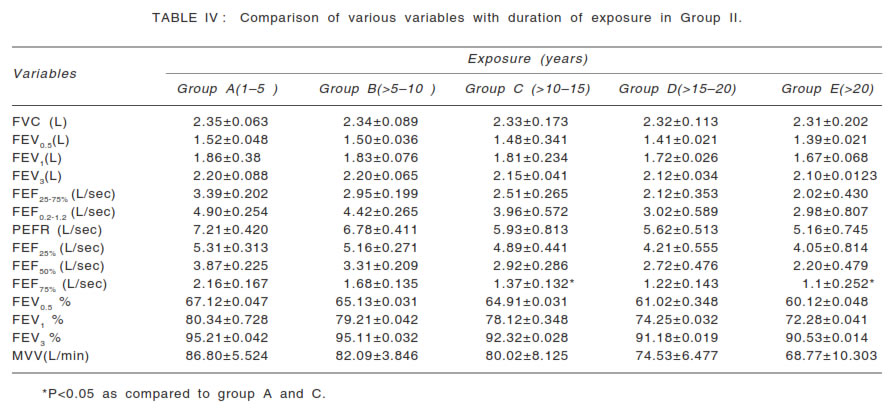
Table IV shows changes in parameters with duration
of exposure in years in group II subjects. As there
was an increase in the duration of exposure in years
there was gradual decline in values of all the
parameters. FVC in group A (duration of exposure 15
years) was found to be 2.35+0.063
L which
decreased gradually as duration of exposure
increased to more than 20 years (2.31+202 L) in group E. However, difference between the categories
was not statistically significant. Similarly FEV,
FEV1, FEV3,
FEF25-75%, PEFR, FEF25%, FEF50%,
FEV0.5 % and FEV1 % were also found to be
decreased as the duration of exposure increased,
however the difference was not statistically
significant. Difference in the value of FEF75% was
found to be statistically significant in subjects with
exposure for 1-5 years (group B) when compared
with groups having duration of exposure as >10-15
years and >20 years. MVV also showed a gradual
decline with a value of 86.80+5.52 L/min in group A
to 68.77+10.30 L/min in group E. |
 |
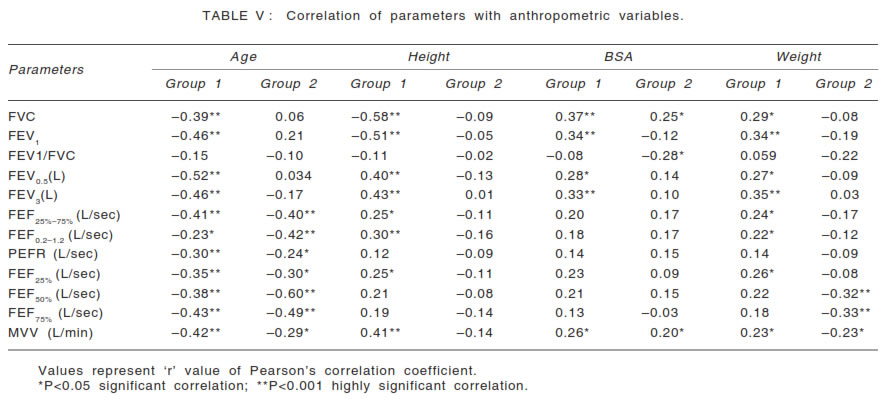 |
There was negative correlation of age with FEV1 and
FVC i.e. there was significant decrease in FEV1 and
FVC with increase in age in control group (Table V).
However, this correlation was not there in group II
consisting of workers. The negative correlation
between age and other flow rates was significant in
both groups. Height had similar negative correlation
with these parameters. BSA and weight had
significant positive correlation with FEV1 and FVC in
group I. |
The demographic profile of subjects in both the groups
was comparable. The height, weight and BSA were
also found to be comparable in both the groups.
Mean age of subjects (33.5 years) was similar to
mean age (34 years) in other studies in industry
workers (19). In Indian scenario, it was expected to
have more number of male workers as compared to
female workers (2). Therefore, in the present studythere was predominance of male workers (87%) as In our study FEV1, FEV1% and FVC were significantly lower in workers as compared to controls. In an earlier study on ginning factory workers, these parameters had lower values in workers (10). FVC and FEV1 % are very important variables in distinguishing restrictive and obstructive lung diseases. A reduced FEV1 % is considered to be the hallmark of obstructive disorder. FEV1 is 80% of the FVC in normal healthy adults. Patients with obstructive lung disease have low flow rates as a result of high airway resistance therefore, their FEV1 % is low. Patients with restrictive lung disease have a reduced FVC but are able to achieve relatively high flow rates therefore, their FEV1 % exceeds 80%. In our study FEV1 % was 79% and 88% in workers and controls, indicating obstructive pulmonary abnormalities in workers. Similar findings were reported in a study done on workers in stone factory where FEV1 % was significantly lower in exposed group than in control group (20). In another study done on ginning (cotton) factory workers, FEV1 % reduced significantly in workers as compared to control group (10). In our study, this decrease was progressively more as the duration of exposure increased. This indicates that in workers of cotton wool industry the respiratory obstructive changes progress with increase in duration of exposure. The other pulmonary flow rates in this study i.e. expiratory flow rates at higher lung volumes (PEFR) and lower lung volumes (FEF25%-75% ) were lower in workers than in controls, but not significantly. Hence, these factors do not provide information on the site of obstruction in our study (11). The importance of percentage predictive values of pulmonary function parameters is more in classifying and diagnosing the type of respiratory disorder than the absolute values alone. The percentage predicted values compare the measured values in relation to a reference value for that specific population using anthropometric indices. In our study, the percentage predicted values of FEV, FVC and MVV were significantly reduced in workers. The percentage predicted FEV1% decreased significantly in male workers as compared to healthy males. The values less than 80% are considered to be indicative of obstructive type of respiratory disorders (7, 16). This is further substantiated by the significant reduction in MVV in workers. MVV demonstrates all mechanical factors of breathing. Decrease in the value of MVV indicates increase in airway resistance, reduced compliance or decreased respiratory muscle force (6, 7, 16). Hence, the findings of the present study indicate obstructive pattern of lung disease. Obstructive diseases are characterized by reduction in ventilation due to increase airflow resistance as a result of blockage of airways by mucosal plugs, narrowing of airway lumen by hypertrophied or inflamed mucosa, bronchoconstriction, loss of elastic recoil and impairment of expiratory flow. All these effects can occur due to inhalation of wool dust leading to obstructive pattern of disease (21). In an earlier study, various flow rates were reduced in carpet workers and this reduction was higher in wool yarn dyers. It indicates that maximum peripheral airway obstruction occurs in wool yarn dyers (22). Gender wise distribution of various variables shows lesser values in female as compared to male subjects. These findings may be explained by the fact that there is greater development of musculo-skeletal system of the thoraco-abdominal compartments as well as that of the pulmonary tissue in men. The parameters like height, weight and body surface area of all subjects were comparable yet the lesser values in females in the present study could be due to differences in the outdoor and occupational habits. Another factor could also be the possible effects of repeated pregnancies in these women. The latter would impair the force of contraction of the abdominal muscles which might restrict the maximal expiratory effort. Another reason for lesser value in females could also be their involvement in cooking thereby getting exposed to indoor air pollution as well. These females are from lower socioeconomic strata and commonly used wood as fuel which yields high quantity of pollutant (23). In our study, we used regression equation which is used for south Indian females. Hence, the results should be interpreted with caution. Not only the type of pollutant but also the duration of exposure to specific pollutant also affects the lung function variables. There was decline in all the parameters as the duration of exposure to wool dust increased but this decline was not found to be statistically significant except for FEF75%. This decline in FEF75% value was significant as duration of exposure increased from 1-5 years to more than 20 years. In a study done on carpet workers, period of occupational exposure was found to be directly related with effects on various respiratory parameters. FEF25%, FEF50%, FEF75% were reduced in all the groups of carpet workers that is in weavers, wool yarn dyers etc (22). There is a direct correlation between the occupational period and the pulmonary abnormalities suggesting that ventilatory impairments are related with duration and nature of the exposure as well. The reason of decline in all the variables with increase in duration of exposure can be due to increase in irritation of upper respiratory tract mucosa due to prolonged exposure to wool dust resulting in hypertrophy of mucosal lining. It results in increased secretion of mucus and formation of mucosal plugs leading to obstruction in exhaled air. However, increasing age in itself can decrease the lung volumes and capacities (11). Textile workers exposed to wool dust for greater than 10 years had similar reduction of ventilatory capacity as those with shorter exposure (24). Differences in various parameters have been attributed to anthropometric differences also. BSA has been considered to be an independent variable for deriving spirometric predictions (15). In our study, there was a decrease in FEV1 and FVC as age increases. The same negative correlation was observed as height increases. Similar association has been reported in earlier studies in healthy volunteers. However, BSA and weight had positive correlation with these parameters in healthy controls (11). This pattern of correlation was found only in control group and not in workers. This indicates that the disease process affects these correlations in workers. Thus, all pulmonary function parameters in workers
in the present study showed reduction in their
values as compared to controls. This indicates
that wool dust at work place accelerated decline in
lung functions. There was also a decrease in the
variables as duration of exposure to wool dust
increased. Hence, it can be concluded from the
results of this study that exposure to wool dust
during wool production in woolen industry is
harmful for the health of the workers. Hence,
preventive steps can be suggested to these workers
and industry. |
|